Modern Virtual Reality Technology: Cybersickness, Sense of Presence, and Gender

Daniel M. Shafer, Ph.D.
Baylor University Department of Film and Digital Media
Corey P. Carbonara, Ph.D.
Baylor University Department of Film and Digital Media
Michael F. Korpi, Ph.D.
Baylor University Department of Film and Digital Media
Abstract
This article reports the results of two experimental studies which investigated 1) differences in how virtual reality (VR) -induced cybersickness is experienced between men and women, and 2) how video game players experience cybersickness when using two generations of developing VR technology. Grounded in sensory conflict theory; the study discusses cybersickness as a function of the differing technical specifications of the VR head-mounted displays (HMDs) used in the experiments.
In Study 1, 223 players played either a first-person shooter or a first-person space flight game on the Oculus Rift DK-1. Results indicated that women experienced more severe cybersickness symptoms than men, and that shooter players experienced more severe symptoms than space flight players. In Study 2, 136 players played Minecraft on either the Oculus Rift DK1 or its successor, the DK2 n m. Players in both headset conditions were compared on cybersickness and sense of presence. Results indicated that the advanced VR technology did not improve the experience of cybersickness or presence over the basic technology. Differences between the headsets were not significant.
Both studies show that cybersickness affects women more than men; however, the reasons for the difference bear further investigation. More importantly, advanced VR technology made no significant difference to users in terms of cybersickness or sense of presence. DK2 users experienced cybersickness symptoms just as severe as their counterparts using the DK1 did. Further research will delve into cybersickness, presence and the newest consumer VR headsets; and will investigate the neuropsychological processes associated with the VR experience.
Acknowledgements: The authors wish to acknowledge the support of the Department of Film and Digital Media at Baylor University.
 Daniel M. Shafer received his Ph.D. from Florida State University in 2009 and is currently Associate Professor of Film and Digital Media at Baylor University. His research interests include the psychological and psysiological effects of new media technology such as virtual reality and innovative control methods; media psychology; video game and other media enjoyment, and morality in media. He is currently involved in several lines of research including the psychological and physiological effects of virtual reality technology the psychological and neurological impact of high frame rate and variable frame rate cinematography, and the emotional and cognitive effects of watching television and film and of using various types of video games. Correspondence should be addressed to: daniel_m_shafer@baylor.edu
Daniel M. Shafer received his Ph.D. from Florida State University in 2009 and is currently Associate Professor of Film and Digital Media at Baylor University. His research interests include the psychological and psysiological effects of new media technology such as virtual reality and innovative control methods; media psychology; video game and other media enjoyment, and morality in media. He is currently involved in several lines of research including the psychological and physiological effects of virtual reality technology the psychological and neurological impact of high frame rate and variable frame rate cinematography, and the emotional and cognitive effects of watching television and film and of using various types of video games. Correspondence should be addressed to: daniel_m_shafer@baylor.edu Corey P. Carbonara received his Ph. D. from the University of Texas at Austin, and is a Professor of Film and Digital Media and Director of the Digital Communication Technologies Project at Baylor University. He is a Senior Research Fellow of the IC2 Institute at UT Austin , and is a Fellow of the Society of Motion Picture and Television Engineers (SMPTE). Dr. Carbonara’s research interests include video games as fluid learning constructs, digital content creation and distribution, digital cinema, IPTV, video game technology and the resulting socio-economic and socio-cultural impacts, wireless mesh sensor networks, digital storage, video compression, creative and innovative management of technology and diffusion of innovations. More recently, Dr. Carbonara was the recipient of the 2013 NAT Tiffen Award for Outstanding Educational Contribution to the Art and Craft of Cinematography, Emerging Cinematographer Award by the International Cinematographers Guild, IATSE 600. He is currently involved in several lines of research including the future applications of augmented reality, the psychological and physiological effects of virtual reality technology, and the psychological and neurological impact of high frame rate and variable frame rate cinematography.
Corey P. Carbonara received his Ph. D. from the University of Texas at Austin, and is a Professor of Film and Digital Media and Director of the Digital Communication Technologies Project at Baylor University. He is a Senior Research Fellow of the IC2 Institute at UT Austin , and is a Fellow of the Society of Motion Picture and Television Engineers (SMPTE). Dr. Carbonara’s research interests include video games as fluid learning constructs, digital content creation and distribution, digital cinema, IPTV, video game technology and the resulting socio-economic and socio-cultural impacts, wireless mesh sensor networks, digital storage, video compression, creative and innovative management of technology and diffusion of innovations. More recently, Dr. Carbonara was the recipient of the 2013 NAT Tiffen Award for Outstanding Educational Contribution to the Art and Craft of Cinematography, Emerging Cinematographer Award by the International Cinematographers Guild, IATSE 600. He is currently involved in several lines of research including the future applications of augmented reality, the psychological and physiological effects of virtual reality technology, and the psychological and neurological impact of high frame rate and variable frame rate cinematography.
 Michael F. Korpi received his PhD from the University of Iowa. He is currently a Professor of Film and Digital Media at Baylor University, a Senior Research Fellow at the IC2 Institute at the University of Texas at Austin, and a Fellow of the Society of Motion Picture and Television Engineers (SMPTE). He has produced and directed documentaries on a range of topics from automobile racing to world hunger. Dr. Korpi also conducts research dealing with new communication technologies, which over the years have included high definition television, nonlinear editing systems, digital cinema, video games, virtual reality (VR), and augmented reality (AR), among others. He is currently involved in several lines of research including the future applications of augmented reality, the psychological and physiological effects of virtual reality technology, and the psychological and neurological impact of high frame rate and variable frame rate cinematography.
Michael F. Korpi received his PhD from the University of Iowa. He is currently a Professor of Film and Digital Media at Baylor University, a Senior Research Fellow at the IC2 Institute at the University of Texas at Austin, and a Fellow of the Society of Motion Picture and Television Engineers (SMPTE). He has produced and directed documentaries on a range of topics from automobile racing to world hunger. Dr. Korpi also conducts research dealing with new communication technologies, which over the years have included high definition television, nonlinear editing systems, digital cinema, video games, virtual reality (VR), and augmented reality (AR), among others. He is currently involved in several lines of research including the future applications of augmented reality, the psychological and physiological effects of virtual reality technology, and the psychological and neurological impact of high frame rate and variable frame rate cinematography.
Introduction
A number of companies are participating in the creation of a consumer market for Virtual Reality (VR) Head-Mounted Displays (HMDs) and the content to view on these displays. Oculus (Facebook), HTC, Samsung, Sony, and Google are prominent in this group. This fresh attempt to develop VR for consumers is largely enabled by advances in technologies originally developed for smartphones, like displays, GPS, low-power processors, GPUs, sensors, and so on. Many are enthusiastic about the prospects for VR, especially Oculus and HTC, who released their consumer devices in early 2016.
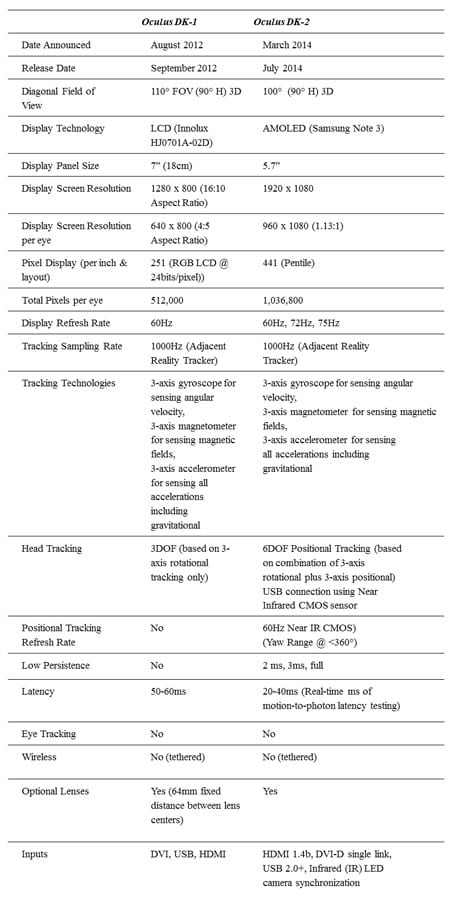
Much of the current enthusiasm for consumer VR is due to high quality and affordable technology now available from the smartphone parts bin (Nield, 2016). Higher resolution, wider viewing angles, better motion tracking, decreased latency, and other advancements promise to significantly improve the VR experience as well as make modern devices more affordable. Thus, many – including developers, technology enthusiasts, and companies like Oculus, Valve, and Sony — have renewed hope that the new form of this technology will revolutionize user engagement and presence in virtual environments. Oculus, in particular, released two development kits intended to encourage the development of software that would work with their technology. Released in 2013, the Oculus Rift DK1, while rudimentary by comparison to currently available commercial HMDs, was a significant achievement. Its successor, the DK2, followed in 2016 and marked a significant advancement as well. Table 1 compares the technical specifications of each headset. The reader will note that at the time of this writing, the primary investigators did not have access to the consumer Oculus Rift or the HTC Vive. More research using these headsets is forthcoming.
Table 1: Oculus Rift DK-1 and DK-2 Virtual Reality System Specification Comparison.
(“Announcing the Oculus Rift Development Kit 2 (DK2),” 2014;
Desai, Desai, Ajmera, & Mehta, 2014; Lang, 2013; Oculus, 2015)
One possible barrier to this VR revolution may be cybersickness. Cybersickness, a term often thought to be interchangeable in popular usage and in the press with “motion sickness,” has symptoms similar to, but not the same as, motion sickness. It has always been an unwelcome factor in VR. In addition, research shows that gender is a factor in cybersickness; females are more likely to experience symptoms (Biocca, 1992). Since women comprise 44% of gamers in the U.S. (“Essential Facts About the Computer and Video Game Industry,” 2014), this gender difference may be particularly problematic for consumer adoption of VR. The present article considers cybersickness and gender in relation to technological improvements between Oculus’s Development Kit 1 and Development Kit 2.
Definition of VR
Virtual reality (VR) is a technology that allows for immersion of a user in a multisensory virtual environment (VE). Using a combination of hardware and software systems, virtual reality creates a three dimensional, interactive world. There are two primary types: CAVE Automatic Virtual Environment (CAVE) and Head Mounted Display (HMD). A CAVE consists of a room with projection screens lining the walls, floor and ceiling. The user typically wears a headset in order to view 3-D imagery in the environment (Rouse, 2016). HMD VR, on the other hand, currently consists of a headset and, for some applications, motion controllers which stand in as proxies for the user’s hands. HMD VR has spurred the recently revived interest in consumer VR, and is the focus of this research. Gigante (1993), writing in Virtual Reality Systems (Earnshaw, Gigante, & Jones, 1993) defines HMD VR as “the illusion of participation in a synthetic environment rather than external observation of such an environment. VR relies on three-dimensional (3D), stereoscopic, head tracked displays, hand/body tracking and binaural sound. VR is an immersive, multi-sensory experience” (p. 3). Although this definition can also be used in describing virtual worlds or environments, in the popular vernacular, VR has come to embody a stereoscopic 3D virtual environment that uses some sort of HMD; either tethered or as a stand-alone device using some sort of mobile device interface.
The fast start of Oculus and the rapid emergence of other VR and AR startups like Magic Leap ($542 million of funding) have been accompanied by announcements of VR and/or AR projects from major corporate players like Google, Sony, Microsoft, and Samsung (Hixon, 2015; Huet, 2014). Despite all this momentum and enthusiasm, there is caution. John Carmack, well-known game designer and CTO of Oculus, referencing the difficulties consumer VR experienced in the 1990s said: “It left a huge, smoking crater in the landscape. We’ve had people afraid to touch VR for 20 years” (Wingfield, 2015).
Cybersickness
One of the primary problems VR has had historically is cybersickness. Cybersickness is a repeatedly observed side effect of VR. There are numerous symptoms associated with cybersickness which include tiredness, drowsiness, nausea, disorientation, postural instability, sweating, headaches, eye strain, and sometimes even vomiting (Burdea & Coiffet, 2003; Davis, Nesbitt, & Nalivaiko, 2014; LaViola, 2000). The issue is complex as there can be variability between individual responses to the stimuli, the type of technology used and the overall design of the virtual environment, and the tasks performed (Davis, Nesbitt, & Nalivaiko, 2015; Johnson, 2005) As Vinson and colleagues (2012) state: “Cybersickness is essentially a barrier to both adoption and production of VR technologies” (p. 69). There are a significant number of studies examining cybersickness in virtual environments (Robert S. Kennedy, Stanney, & Dunlap, 2000; LaViola, 2000; Stanney & Hash, 1998; Vinson et al., 2012).
Cybersickness can be caused solely by visual input (LaViola, 2000). Vestibular stimulation is often absent in occurrences of cybersickness because the individual is sitting still, and therefore there may be a significant mismatch between movement in the VE and the lack of movement from sitting. This visual versus vestibular conflict results in an experience known as vection (LaViola, 2000). Vection is the experience of self-motion even when you are not actually moving. As So, Ho and Lo (2001) put it, vection is a “visually induced self-motion illusion” (p. 195). Many of us have experienced vection in the real world; while sitting at a traffic light next to a large truck, you suddenly feel like you are moving backwards. In reality, the truck’s wheel, which fills your field of view to the side, is moving forward slightly (LaViola, 2000; Riecke, Väljamäe, & Schulte-Pelkum, 2009). Vection, then, is one contributor to cybersickness symptoms, but it is insufficient to predict cybersickness in all cases. Several theories have been posited that attempt to predict the conditions under which cybersickness will occur. Three of the leading perspectives are poison theory (LaViola 2000; Kennedy and Frank 1985), postural instability theory (Riccio and Stoffregen 1991), and sensory conflict theory (Brand 1978; Reason and Brand 1975).
Poison Theory
Poison theory posits that when the body encounters events that cause dissonance between what is felt and what is being processed visually, the central nervous system interprets this dissonance as toxic (Kennedy and Frank, 1985).. This perception of toxicity is thought to bring about symptoms of motion sickness. As LaViola (2000) puts it, poison theory suggests that the body reacts to the ingestion of poison by disrupting the coordination between the visual and vestibular systems (among others). One natural reaction to this disruption is to vomit; which also serves as a way to expel the toxic substance that has been ingested (LaViola 2000). For the purposes of this study, we do not consider the poison theory applicable, since it cannot predict who will become ill to the point of vomiting, and cannot explain why some experience sickness symptoms, and others do not (LaViola 2000).
Postural Instability Theory
The postural instability theory proposed by Riccio and Stoffregen (1991) posits that motion sickness occurs when an entity (human or animal) experiences a loss of posture control. The theory is based in work on control of self-motion and orientation, and is a departure from sensory conflict theory which focuses on motion-sensing systems such as the vestibular system. To put it very simply; if postural instability (the feeling that one is not in control of their own motion or orientation) is prolonged, motion sickness will occur. Riccio and Stoffregen (1991) categorically reject the arguments of Reason and Brand (1975) which attempt to explain motion sickness; instead proposing that motion sickness stems from loss of motion control. However, it seems to us that sensory conflict theory is more suited to explaining the phenomenon of cybersickness than postural instability theory, because many experiences of cybersickness occur when the body is at rest, not in motion. Results of research investigating postural instability theory have been mixed (e.g., Smart et al 2002; Wang Kenyon and Keshner 2010), but recent research shows that the relationship between postural instability and cybersickness is weak in some cases (Dennison and D’Zmura 2017) We therefore turn to sensory conflict theory and our application of it to the investigation of cybersickness.
Sensory Conflict Theory
Sensory conflict theory (Reason, 1978; Reason & Brand, 1975) was proposed in order to predict incidence and severity of motion sickness. The basic principle of the theory asserts that motion sickness is likely to occur when motion sensing systems (namely the eyes, the vestibular system, and the nonvestibular proprioceptors) send signals that conflict with 1) each other or 2) what is expected based on previous experiences (Bles, Bos, de Graaf, Groen, & Wertheim, 1998). According to the theory, motion sickness occurs when a person fails to experience an expected physiological response to a certain visual stimulus (Reason, 1978). Relevant examples for the purposes of the present study might be using a VR flight simulator or a driving simulator that includes a great deal of surrounding movement. Turning one’s head in such an environment may result in a conflict between the visual input and what one’s brain would normally expect in real flight or driving because the simulator is fixed in place. The same conflict might be expected when playing a first-person shooter video game or a space dogfighting game in VR. This is because in reality, you are sitting still in a chair, while your avatar in-game appears to be making rapid movements or moving through space quickly. The strength of the motion sickness response, Reason (1978) argues, is dependent upon 1) how severe the conflict is between the perceived and expected stimulus, and 2) exposure time to the same stimulus. The thrust of Reason’s (1978) argument is that symptoms of sickness can be reduced by adaptation to the conflict perceived between the observed visual stimulus and expected result of exposure to such stimulus (Reason, 1978).
While we may expect, then, that VR video game players might experience fewer symptoms the longer they play, this may, in fact, be unlikely. Video game scenery and events change constantly, while the stimulus material Reason (1978) used was repetitive and constant. In a video game, player attention can be drawn suddenly to diverse portions of the display, causing sudden and erratic head and even body motion. Therefore, it is more unlikely that VR video game players would become accustomed to the environment and experience reduced cybersickness systems simply due to exposure time. However, based on the arguments of sensory conflict theory, we might expect that games which produce more conflict between the motion-detecting senses and the player’s expectations will be more sickness-inducing than games in which the motion experienced and expected is more congruent. Reason (1978) asserted that the brain compares incoming motion stimuli (e.g., immersive visual information) with previous responses experienced under similar real-life conditions, now stored in a memory bank of “paired sensory and motor memory traces” (Oman, 1993, p. 365). When the signals received do not align with the stored memory trace of that stimulus, sensory conflict results. The longer one experiences this sensory conflict, the more likely sickness is to occur. However, it is not possible to measure the level of conflict between the senses and the physiological expectations an individual is experiencing.
Oman (1993) developed a mathematical formula designed to determine the intensity of sickness responses based on a variety of measurable factors. The key element in both Oman’s (1993) and Reason’s (1978) work is that the more the stimuli (e.g., the visual stimuli produced by a VR video game) sends motion cues that are expected (by our physiological systems) to produce certain responses but in fact do not, the more severe cybersickness systems are likely to be. “Increased sensory conflict is noted to result not only from sensory rearrangement but also from exogenous disturbance forces acting on the body” (Oman, 1993, p. 367). These exogenous disturbance forces could be an involuntary movement made in response to intense or surprising visual or auditory stimuli; which are common in action-packed video games.
Still, different VR games may produce widely varying levels of sensory conflict. Some games, such as a virtual hunting game, for instance, would be unlikely to produce a great deal of sensory conflict because the action on screen and the visual stimulus provided would generally match with what the body might expect in real life. Similarly, a flight simulator may not produce extraordinary sensory conflict because the player’s avatar is seated in a cockpit, with the action taking place around it. Being seated in real life would lend some degree of similarity between the virtual and the real world. However, a first-person shooter, with a great deal of running and turning, should produce a high level of sensory conflict because of the discrepancy between the running action on screen and being seated in a chair in real life
Therefore, we predict that:
H1: A VR video game that is higher in sensory conflict (i.e., a first-person shooter) will produce more cybersickness symptoms in players than a VR video game that is lower in sensory conflict (i.e., a space dogfighting game).
Cybersickness and Gender
The finding that women are more susceptible to cybersickness symptoms than men is common in the VR literature. In fact, one study only used men as test subjects in order to better isolate the effects of VR on cybersickness (Lo & So, 2001). A study by Kim and colleagues (2005) reported that over 78% of participants who reported cybersickness symptoms were women. Kennedy and Frank (1985) and Biocca (1992) also note that women are more likely to experience cybersickness than their male counterparts. In one study, cybersickness scores were obtained after exposing participants to either a virtual environment that provided coaching and direction intended to relieve or blunt the onset of cybersickness symptoms (a cybersickness relief virtual environment, or CRVE); or by having participants use a non-CRVE environment (Kim et al., 2008). Women in the study reported significantly greater cybersickness than men across conditions; in fact, the average female cybersickness frequency score was over two times greater (10.5 times during exposure) than the average male frequency score (4.1). This means that women expressed feelings of cybersickness verbally an average of 10.5 times during their exposure, whereas men verbally expressed their symptoms an average of 4.1 times during exposure (Kim et al., 2008). Another study by Stanney and colleagues (2003) analyzed men and women’s scores on the subscales of the SSQ. They found that women experienced significantly higher levels of disorientation, oculomotor symptoms, and higher total severity scores than men did. Men and women did report similar levels of nausea in that study (Stanney et al., 2003).
On the other hand, a few studies have found that women and men do not differ in their experience of cybersickness in VR. Knight and Arns (2006) report that men and women experienced similar levels of cybersickness in the CAVE virtual reality environment. Larson and colleagues (1999), in their study of men and women’s performance in a virtual reality spatial rotation (VRSR) test, found that men and women did not differ in their post-exposure cybersickness symptoms. Other studies (e.g., Bonato, Bubka, & Palmisano, 2009; Howarth & Finch, 1999; Stanney & Hash, 1998) simply do not mention gender as a factor. Given this evidence, it would appear that, despite some mixed results, women generally experience cybersickness more frequently and/or more severely than men while using VR. Therefore, it is predicted that:
H2: Women will score higher than men across conditions on a measure of post-exposure cybersickness after playing a VR video game.
In order to test these hypotheses, data was collected via a 2 condition randomized between-subjects experiment (see Shadish, Cook, & Campbell, 2002).
This research re-examines cybersickness with the latest readily available VR technology, the Oculus Rift. (We used Oculus in favor of other VR HMDs because two distinct generations were available to developers and scholars such as ourselves.) We also re-examine the notion that women are more susceptible to cybersickness than men. In addition, we empirically test the notion that advanced VR technology reduces cybersickness and increases the sense of presence for users. To these ends, this study employs Developer Kit Version 1 (DK-1) and Developer Kit Version 2 (DK-2). Table 1 describes the technical specifications of each headset.
Study 1 Methodology
Participants in Study 1 were 223 undergraduate students recruited via email and Internet announcements from various courses at a research university in the southern-central United States. Participants were offered extra credit for their participation, among other options for extra credit. The gender breakdown for the sample was 48.4% male (n = 108) and 51.6% female (n = 115). Average age was 20.4 years. Participants were randomly assigned to play either a first-person shooter (Half Life 2) or a space dogfighting video game (Strike Suit Zero) using a VR HMD – the Oculus Rift DK-1.
Stimulus and Systems
Via random assignment, participants were selected to play in one of two conditions. The high sensory conflict condition utilized Half Life 2. The game involves navigating through an obstacle-laden virtual environment. The avatar in the game walks or runs through the environment, and the hand or weapon that is recognizable as the player’s own digital self in the game makes a “bobbing” motion as movement takes place. Players played a portion of the game which involved navigating through an area with obstacles, and finally engaging some hostile non-player characters (NPCs) in combat with various weapons. Players are able to command the avatar to move forward, backward, side-to-side, and up and down. The HMD gives them the freedom to look in a 180-degree arc to either side, potentially giving a 360-degree view of the environment no matter what the avatar is doing.
The low sensory conflict condition utilized Strike Suit Zero. The game involves flying a space fighter to various coordinates, doing target practice on space junk, and finally, engaging hostile NPCs’ ships in a dogfight. The avatar in the game sits still in the cockpit of the ship. Its hands grip the control sticks, and its legs are visible and unmoving. Pitch, roll, and yaw are all represented in the game, and the player is able to fly their ship in any direction. As with Half Life 2, the HMD gave players the ability to look in a 180-degree arc to either side, potentially giving a 360-degree view of the environment. However, it is clearly represented that the avatar is sitting motionless in the cockpit of a ship.
Procedure
After giving informed consent, participants were asked to watch a 5-minute video tutorial (Half Life 2) or follow a built-in tutorial for the game (Strike Suit Zero). The function of each tutorial was to explain the controls of the game and how to make progress. Upon completion of the tutorials, players played the game for 20 minutes. Immediately after exposure, participants were directed to the 30-question online questionnaire which assessed their level of cybersickness, spatial presence, and demographics. Total experiment time was approximately 45 minutes.
Measures
Cybersickness was assessed using the negative feelings subscale of the ITC-Sense of Presence Inventory (Lessiter, Freeman, Keogh, & Davidoff, 2001). The subscale assesses the level of virtually all symptoms of cybersickness. Specifically, the items measured disorientation, tiredness, dizziness, eyestrain, headache, and nausea on a 5-point Likert-type scale. While these may not cover the entire scope of symptoms of cybersickness, they certainly assess those symptoms that are most salient to players (Kolasinski, 1995; Lang, 2013; LaViola, 2000). This measure had an observed Cronbach’s α = .86. Gender was assessed via a simple single-item question: “Sex”, with “Male” and “Female” as answer choices.
Study 1 Results
Hypothesis 1 predicted that a high sensory conflict VR game (Half-Life 2, a first-person shooter) would produce more cybersickness symptoms in players than a low sensory conflict VR game (Strike Suit Zero, a space dogfighting game). Results of a one-way analysis of variance (ANOVA) show that H1 was supported. Half-Life 2 players experienced significantly higher levels of cybersickness (M = 4.02, SD = 0.91) than Strike Suit Zero players (M = 3.30, SD = 0.94), F (1, 210) = 31.54, p < .001, η2part = .13. Results of Levene’s test of equality of error variances indicated that error variances were statistically equal across groups, F (1, 210) = 2.68, p = .103.
A follow-up ANOVA analyzed players according to gender. Results indicated that men who played Half-Life 2 reported significantly more cybersickness (M = 3.68, SD = 1.05) than men who played Strike Suit Zero (M = 3.01, SD = 0.95), F (1, 100) = 11.03, p = .001, η2part = .10 (Levene’s F (1, 100) = 0.001, p = .970). Women who played Half-Life 2 reported significantly more cybersickness (M = 4.30, SD = 0.67) than women who played Strike Suit Zero (M = 3.59, SD = 0.83), F (1, 108) = 23.88, p < .001, η2part = .18. For the women, Levene’s test was significant (F (1, 108) = 4.46, p = .037), indicating unequal error variances, however GLM procedures including ANOVA are robust to violations of the equal error variances assumption when group sizes are relatively equal (Howell, 2012). For this test, 51 women were in the Half-Life 2 condition and 59 women were in the Strike Suit Zero condition. Half-Life 2 produced more cybersickness both generally and when broken down by gender.
Hypothesis 2 predicted that women would report higher levels of cybersickness than men in both the high sensory conflict (Half-Life 2) and low sensory conflict (Strike Suit Zero) conditions. Results of a one-way ANOVA show that H2 was supported. Women who played Half-Life 2 reported significantly more cybersickness (M = 4.30, SD = 0.67) than men who played Half-Life 2 (M = 3.68, SD = 1.05), F (1, 91) = 12.03, p = .001, η2part = .12 (Levene’s F (1, 91) = 6.28, p = .014). Women who played Strike Suit Zero reported significantly more cybersickness (M = 3.59, SD = 0.83) than men who played Strike Suit Zero (M = 3.01, SD = 0.96), F (1, 117) = 12.30, p = .001 η2part = .10 (Levene’s F (1, 117) = 1.32, p = .252). However, further follow-up correlation analysis revealed that playing computer games more often is negatively related to cybersickness (r = -0.28, p < .001), as is knowledge of how VR works (r = -0.19, p = .005). Those with more gaming experience and more in-depth knowledge of how VR works tended to experience less severe cybersickness than their counterparts.
Study 2: Cybersickness and VR Technology
In Study 1 we investigated the problem of cybersickness as it relates to virtual reality. In Study 2, we focus on the potential for improvements in VR technology to reduce the symptoms of cybersickness. The general notion among VR device developers is that a higher resolution display, increased framerate, increased refresh rate, decreased latency, and a low persistence display will all contribute to reduced cybersickness. As of the writing of this article, there were only two available headsets that allow a direct comparison of these factors: the Oculus Rift DK-1 and DK-2. In all cases, the DK-2 is superior technologically. Table 1 compares the technical specifications of the two headsets, and demonstrates that the DK-2 outstrips the DK-1 in each area of interest (as it was designed to do).
What cannot be said simply by looking at the technical specifications is how users react to VR experiences using the DK-2 as compared to the DK-1. In order to make such a comparison, we designed an experiment that held the virtual environment and control method constant, and only varied the Oculus Rift version used by the participants.
Our primary goal for this experiment was to determine if DK-2 produced significantly less cybersickness than DK-1, as the technological advancements suggest it should. Oculus developers themselves that the DK-2 would reduce cybersickness in their announcement of the release of the device: “Like the Crystal Cove prototype, DK-2 uses a low persistence OLED display to eliminate motion blur and judder, two of the biggest contributors to simulator sickness. Low persistence also makes the scene appear more visually stable, increasing the potential for presence” (“Announcing the Oculus Rift Development Kit 2 (DK2),” 2014). Therefore, we propose the following hypotheses:
H3: Users of the Oculus Rift DK-1 will report significantly more cybersickness than users of the DK-2.
H4: Users of the DK-2 will report significantly higher levels of spatial presence than users of the DK-1.
H5: Users of the Oculus Rift DK-1 will drop out of the study significantly more frequently than users of the DK-2.
Study 2 Methodology
Participants in Study 2 were 136 undergraduate students recruited via email and digital announcements from various courses at a research university in the southern-central United States. Participants were offered extra credit for their participation, among other options for extra credit. The gender breakdown for the sample was 56% male (n = 76) and 44% female (n = 60). Average age was 20.6 years. Via random assignment, 56.6% of participants were assigned to the DK-1 condition, and 43.6% of participants were assigned to the DK-2 condition.
Stimulus and Systems
The technical specifications of the DK-1 and the DK-2 have been summarized in Table 1. The two headsets comprised the two conditions for the experiment. Participants played a modified version of the popular sandbox game Minecraft . Minecraft was chosen as stimulus material for this study (just as Half Life 2 and Strike Suit Zero were chosen for Study 1). Specifically, participants played Minecrift 1.7.10 Pre5; a modification of Minecraft that adapts the game for use with the Oculus Rift DK-2, and is backward compatible with the DK-1. The participants were randomly assigned to play using the DK-1 (basic VR) or the DK-2 (advanced VR). They played in a pre-constructed tutorial world originally created for MinecraftEdu. The tutorial world is a valid stimulus for both experienced players and players new to Minecraft, because it covers all the basics of the mechanics of the game, yet is in-depth enough to offer experienced players small challenges to complete as they make their way through the environment.
Players controlled their avatar using an XBOX 360 USB controller, which interfaced with Minecraft via a piece of software called Keysticks (Keysticks.net n.d.). Keysticks allows users to customize each button on the controller. Using an XBOX 360 controller allowed players to control their avatars without the need to look at their hands on the keyboard; particularly useful when using a visually occlusive VR HMD like the Oculus Rift.
Procedure
After giving informed consent, participants were asked to play Minecraft in VR for 20 minutes. They were told they could end their participation at any time for any reason. Sixty-six participants (37.5%) reported that they ended their play session early (4.7% did not answer the question). Ending the play session early was positively and significantly associated with cybersickness scores (r = .383, p < .01), indicating that cybersickness symptoms may have been related to ending play sessions early.
Measures
Spatial presence was measured using the Spatial Presence subscale of the ITC-Sense of Presence Inventory (ITC-SOPI; Lessiter et al., 2001). Some example items include: “I had a sense of being in the scenes displayed”; “I felt as though I was in the same space as the characters and/or objects”; “I felt surrounded by the displayed environment”. Observed Cronbach’s α = .92.
Cybersickness was assessed using the Simulator Sickness Questionnaire (Robert S. Kennedy, Lane, Berbaum, & Lilienthal, 1993). This measure improves upon the negative feelings portion of the ITC-SOPI in measuring possible negative reactions to virtual reality environments. The scale had an observed Cronbach’s α = .93. Gender was assessed via a simple single-item question: “Sex”, with “Male” and “Female” as answer choices.
Study 2 Results
The hypotheses for Study 2 were tested using an analysis of variance (ANOVA) procedure. Hypothesis 3 predicted that DK-1 users would experience higher levels of cybersickness than DK-2 users. The results indicate that H3 was not supported. DK-1 users reported an average cybersickness score of 0.93 (on a scale from 0-3, SD = 0.64), while DK-2 users reported an average score of 0.78 (SD = 0.66). This difference was not statistically significant, F(1, 134) = 1.79, p = 0.18, η2part = .013 (Levene’s F(1, 134) = .051, p = 0.82).
Hypothesis 4 predicted that DK-2 users would experience significantly higher levels of spatial presence than users than DK-1 users. This hypothesis was also not supported. DK-2 users (M = 3.44, SD = 0.60) did not experience a significantly greater sense of spatial presence than DK-1 users (M = 3.42, SD = 0.64), F(1, 134) = 0.02, p = 0.90 η2part = .00 (Levene’s F(1, 134) = .035, p = 0.85).
Hypothesis 5 predicted that DK-1 users would drop out of the study significantly more frequently than DK-2 users. A frequencies comparison indicated that both conditions had nearly the same dropout rate. For DK-1 users, 36.4% reported that they had to end their play session early, while 39% of DK-2 users reported having to drop out early. A t-test analysis indicated that these values were not significantly different t = -0.311, p = 0.76. H5 is not supported.
Follow-up ANOVA analyses were conducted to explore possible alternative explanations of cybersickness. Comparisons were made based on gender, which Study 1 indicated is an important factor in understanding cybersickness. We also compared players with experience playing Minecraft and games like it with those without such experience. Results of the gender comparison indicate that males reported significantly less severe cybersickness symptoms (M = 0.74, SD = 0.66) than women (M = 1.03, SD = 0.61), F(1, 134) = 7.01, p = .009 η2part = .05 (Levene’s F(1, 134) = .603, p = 0.44). However, gender only explained about 5% of the variance in cybersickness, indicating several other factors at play. In terms of previous exposure, players who had previously played Minecraft reported significantly less severe cybersickness symptoms (M = 0.70, SD = 0.62) than those who had not (M = 1.03, SD = 0.64), F(1, 134) = 9.02, p = .003. Players who had played a game similar to Minecraft before reported significantly less severe cybersickness symptoms (M = 0.71, SD = 0.65) than those who had not (M = 1.00, SD = 0.62), F(1, 134) = 7.27, p = .008 η2part = .06 (Levene’s F(1, 133) = .488, p = 0.49). Previous exposure also explained a small portion of the variance (6%) in cybersickness scores.
Discussion
In this article, we have investigated how players react to playing games in virtual environments; both from an individual differences (i.e., gender) and a technological standpoint. Results of our first experiment show that a high sensory conflict game (Half Life 2) produced more severe cybersickness symptoms than a low sensory conflict game (Strike Suit Zero). This finding supports our arguments that sensory conflict theory as formulated by Reason and Brand (1975) and modified by Oman (1993) can help explain the occurrence and severity of cybersickness.
Our results also show that women experience higher levels of cybersickness than men in both low sensory conflict and high sensory conflict games. However, it is unclear that the difference can simply be explained away by gender. In fact, our follow-up analysis suggests that video game playing experience and previous knowledge of how VR works (or the lack thereof) may contribute to cybersickness just as much as gender. These findings resonate with past research on gender differences and video game performance (Brown, Hall, Holtzer, Brown, & Brown, 1997) which suggests that men perform better in video game competitions than women across a variety of conditions. In fact, susceptibility or resistance to cybersickness may stem from life experiences that are merely associated with typical (or stereotypical) gender roles such as participation in sports (Selby & Lewko, 1976). Some research suggests that athletes develop better object tracking skills than non-athletes; which transfers well to skillful video game play (Cavanagh & Alvarez, 2005). Other research by NASA suggests that familiarity and experience with motion-sickness causing stimuli reduces symptoms during spacecraft test flights (Cowings, Toscano, Reschke, Gebreyesus & Rocha, 2017). This study aligns with our findings that familiarity with cybersickness-inducing VR games helps to mitigate cybersickness symptoms. Such considerations are rich ground for future research.
Findings of our second experiment have serious implications for VR developers. We designed the study to determine whether the technological improvements of the Oculus Rift DK-2 over the DK-1 would improve user’s experiences in terms of cybersickness. Our findings show that despite the evolution of VR technology used in the DK-2 over the DK-1, this made no significant difference to users in terms of cybersickness. Users of the DK-2 experienced cybersickness symptoms just as severe as their counterparts using the DK-1. The DK-2 also failed to produce a greater sense of spatial presence than the DK-1. In fact, users of both headsets reported the same rate of dropout during their play sessions. For all intents and purposes, the two headsets seemed to perform nearly the same in terms of cybersickness and spatial presence.
Limitations
One notable limitation to our study is that none of the games used were originally designed with the Oculus Rift in mind. Instead, all three games utilized in these experiments were retrofitted to support the binocular display of the Rift. It is possible that other games, designed to work natively with the Oculus Rift DK-1 or DK-2 would have produced better user experiences, or perhaps more distinct differences between DK-1 and DK-2 users. However, in experiment 1, users reported very similar experiences between high and low sensory conflict games; indicating that games of different types and (arguably) different quality produce similar user experiences. Further, simply from an anecdotal standpoint, the adaptations of all three games (Half Life 2, Strike Suit Zero, and Minecraft) were very good. The representations of the environments as displayed in the Oculus Rift’s field of view were seamless. The only moments of strangeness may have been when players moved their heads in certain extreme ways while using the DK-2, their in-game avatars appeared as decapitated bodies. This was no doubt due to the Oculus DK-2’s ability to sense depth and movement along the Z-axis. The avatar’s bodies, particularly in Strike Suit Zero and Minecraft, failed to respond to movement along the Z-axis. This may have caused some discomfort for players that may not have been experienced in games specifically designed for the Oculus Rift.
One additional consideration here is that there may be a certain technological threshold where technology ceases to make a significant impact of users’ sense of cybersickness. It is possible that both headsets used in this study exceed that threshold. Finally, we were also unable to manipulate frame rate to truly test the DK-2’s latency reduction capability.
Conclusions and Future Research
Despite these limitations, our results have a few implications. First, we may be seeing evidence that men and women experience different degrees of cybersickness due to the physiological differences in the way the eye and brain process the VR experience. This finding leads us to advocate for more research to test for these differences. In addition, work needs to be done across more samples of emerging VR technology. Consumer versions of the Oculus Rift, the HTC Vive, and the Sony PSVR have now been released, and other competitors are close to unleashing their products.
It will soon be possible to judge whether claims that the issue of cybersickness has been solved are valid. Not only are we determined to continue our work in this realm, but we are now poised to venture into the investigation of the motion imaging characteristics of games designed specifically for the newest VR HMDs (such as Lucky’s Tale; “Playful,” n.d.), as well as VR narratives and simulations.
References
Announcing the Oculus Rift Development Kit 2 (DK2). (2014). Retrieved July 21, 2015, from https://www.oculus.com/blog/announcing-the-oculus-rift-development-kit-2-dk2
Biocca, F. (1992). Will Simulation Sickness Slow Down the Diffusion of Virtual Environment Technology? Presence: Teleoperators and Virtual Environments, 1(3), 334–343. https://doi.org/10.1162/pres.1992.1.3.334
Bles, W., Bos, J. E., de Graaf, B., Groen, E., & Wertheim, A. H. (1998). Motion sickness: only one provocative conflict? Brain Research Bulletin, 47(5), 481–487. https://doi.org/10.1016/S0361-9230(98)00115-4
Bonato, F., Bubka, A., & Palmisano, S. (2009). Combined Pitch and Roll and Cybersickness in a Virtual Environment. Aviation, Space, and Environmental Medicine, 80(11), 941–945. https://doi.org/10.3357/ASEM.2394.2009
Brand, J. . (1978). Motion sickness adaptation: A neural mismatch model. Journal of the Royal Society of Medicine, 71, 819–829.
Brown, R. M., Hall, L. R., Holtzer, R., Brown, S. L., & Brown, N. L. (1997). Gender and Video Game Performance. Sex Roles, 36(11–12), 793–812. https://doi.org/10.1023/A:1025631307585
Burdea, G., & Coiffet, P. (2003). Virtual Reality Technology. Presence: Teleoperators and Virtual Environments, 12(6), 663–664. https://doi.org/10.1162/105474603322955950
Cavanagh, P., & Alvarez, G. A. (2005). Tracking multiple targets with multifocal attention. Trends in Cognitive Sciences, 9(7), 349–354. https://doi.org/10.1016/j.tics.2005.05.009
Cowings, P. S., Toscano, W. B., Reschke, M. F., Gebreyesus, F., & Rocha, C. (2017). Autogenic-feedback training exercise (AFTE) mitigates the effects of spatial disorientation to simulated orion spacecraft re-entry: Individual differences. NASA Technical Report. Retrieved 8/17/2017 from https://ntrs.nasa.gov/search.jsp?R=20170006194
Davis, S., Nesbitt, K., & Nalivaiko, E. (2014). A Systematic Review of Cybersickness. In Proceedings of the 2014 Conference on Interactive Entertainment (p. 8:1–8:9). New York, NY, USA: ACM. https://doi.org/10.1145/2677758.2677780
Davis, S., Nesbitt, K., & Nalivaiko, E. (2015). Comparing the onset of cybersickness using the Oculus Rift and two virtual roller coasters. In Proceedings of the 11th Australasian Conference on Interactive Entertainment. Sydney, Australia: Australian Computer Society. Retrieved from http://crpit.com/confpapers/CRPITV167Davis.pdf
Desai, P. R., Desai, P. N., Ajmera, K. D., & Mehta, K. (2014). A Review Paper on Oculus Rift-A Virtual Reality Headset. International Journal of Engineering Trends and Technology, 13(4), 175–179.
Earnshaw, R. A., Gigante, M. A., & Jones, H. (1993). Virtual Reality Systems. Academic Press.
Essential Facts About the Computer and Video Game Industry. (2014). Retrieved April 6, 2015, from http://www.theesa.com/wp-content/uploads/2014/10/ESA_EF_2014.pdf
Gigante, M. (1993). Virtual Reality: Definitions, History, and Applications. In R. A. Earnshaw, M. Gigante, & H. Jones (Eds.), Virtual Reality Systems (pp. 3–14). London: Academic Press.
Hixon, T. (2015). Virtual Reality Is Hot, But Is It Real? Retrieved June 23, 2015, from http://www.forbes.com/sites/toddhixon/2015/03/20/is-virtual-reality-for-real/
Howarth, P. A., & Finch, M. (1999). The nauseogenicity of two methods of navigating within a virtual environment. Applied Ergonomics, 30(1), 39–45.
Howell, D. C. (2012). Statistical Methods for Psychology. Cengage Learning.
Huet, E. (2014, October 21). Google Leads Monster $542 Million Funding For Magic Leap, A Mysterious “Cinematic Reality” Company – Forbes. Retrieved August 25, 2016, from http://www.forbes.com/sites/ellenhuet/2014/10/21/google-leads-monster-542-million-funding-for-magic-leap-a-mysterious-cinematic-reality-company/#756d27077656
Johnson, D. M. (2005). Introduction to and review of simulator sickness research. DTIC Document. Retrieved from http://oai.dtic.mil/oai/oai?verb=getRecord&metadataPrefix=html&identifier=ADA434495
Kennedy, R. S., & Frank, L. H. (1985). A Review of Motion Sickness with Special Reference to Simulator Sickness. CANYON RESEARCH GROUP INC WESTLAKE VILLAGE CA. Retrieved from http://oai.dtic.mil/oai/oai?verb=getRecord&metadataPrefix=html&identifier=ADA155975
Kennedy, Robert S., Lane, N. E., Berbaum, K. S., & Lilienthal, M. G. (1993). Simulator Sickness Questionnaire: An Enhanced Method for Quantifying Simulator Sickness. The International Journal of Aviation Psychology, 3(3), 203–220. https://doi.org/10.1207/s15327108ijap0303_3
Kennedy, Robert S., Stanney, K. M., & Dunlap, W. P. (2000). Duration and Exposure to Virtual Environments: Sickness Curves During and Across Sessions. Presence: Teleoperators and Virtual Environments, 9(5), 463–472. https://doi.org/10.1162/105474600566952
Kim, Y. Y., Kim, E. N., Park, M. J., Park, K. S., Ko, H. D., & Kim, H. T. (2008). The Application of Biosignal Feedback for Reducing Cybersickness from Exposure to a Virtual Environment. Presence: Teleoperators and Virtual Environments, 17(1), 1–16. https://doi.org/10.1162/pres.17.1.1
Kim, Y. Y., Kim, H. J., Kim, E. N., Ko, H. D., & Kim, H. T. (2005). Characteristic changes in the physiological components of cybersickness. Psychophysiology, 42(5), 616–625. https://doi.org/10.1111/j.1469-8986.2005.00349.x
Knight, M. M., & Arns, L. L. (2006). The relationship among age and other factors on incidence of cybersickness in immersive environment users. In ACM SIGGRAPH 2006 Research posters (p. 196). ACM. Retrieved from http://dl.acm.org/citation.cfm?id=1179846
Kolasinski, E. M. (1995). Simulator sickness in virtual environments (No. ARI-TR-1027). Army Research Inst. for the Behavioral and Social Sciences.
Lang, B. (2013, February 24). John Carmack Talks Virtual Reality Latency Mitigation Strategies. Retrieved August 25, 2016, from http://www.roadtovr.com/john-carmack-talks-virtual-reality-latency-mitigation-strategies/
Larson, P., Rizzo, A. a., Buckwalter, J. g., Van Rooyen, A., Kratz, K., Neumann, U., … Van Der Zaag, C. (1999). Gender Issues in the Use of Virtual Environments. CyberPsychology & Behavior, 2(2), 113–123. https://doi.org/10.1089/cpb.1999.2.113
LaViola, J. J. (2000). A discussion of cybersickness in virtual environments. ACM SIGCHI Bulletin, 32(1), 47–56.
Lessiter, J., Freeman, J., Keogh, E., & Davidoff, J. (2001). A cross-media presence questionnaire: The ITC-sense of presence inventory. Presence: Teleoperators and Virtual Environments, 10(3), 282–297. https://doi.org/10.1162/105474601300343612
Lo, W. T., & So, R. H. (2001). Cybersickness in the presence of scene rotational movements along different axes. Applied Ergonomics, 32(1), 1–14.
Nield, D. (2016, March 29). How Oculus Rift works: Everything you need to know about the VR sensation. Retrieved February 28, 2017, from https://www.wareable.com/oculus-rift/how-oculus-rift-works
Oculus. (2015). Best Practices Guide.
Oman, C. M. (1993). Sensory conflict in motion sickness: An observer theory approach. In S. R. Ellie (Ed.), Pictorial communication in virtual and real environments (pp. 362–375). London: Taylor & Francis.
Playful. (n.d.). Retrieved September 11, 2015, from http://playfulcorp.com/#lucky
Reason, J. T. (1978). Motion sickness adaptation: a neural mismatch model. Journal of the Royal Society of Medicine, 71(11), 819.
Reason, J. T., & Brand, J. J. (1975). Motion Sickness (1st ed.). London: Academic Press.
Riccio, G. E., & Stoffregen, T. A. (1991). An ecological Theory of Motion Sickness and Postural Instability. Ecological Psychology, 3(3), 195–240. https://doi.org/10.1207/s15326969eco0303_2
Riecke, B. E., Väljamäe, A., & Schulte-Pelkum, J. (2009). Moving sounds enhance the visually-induced self-motion illusion (circular vection) in virtual reality. ACM Transactions on Applied Perception, 6(2), 1–27. https://doi.org/10.1145/1498700.1498701
Rouse, M. (2016) CAVE (Cave Automatic Virtual Environment). Techtarget. Retrieved 8/13/2017 from http://whatis.techtarget.com/definition/CAVE-Cave-Automatic-Virtual-Environment
Selby, R., & Lewko, J. H. (1976). Children’s Attitudes toward Females in Sports: Their Relationship with Sex, Grade, and Sports Participation. Research Quarterly. American Alliance for Health, Physical Education and Recreation, 47(3), 453–463. https://doi.org/10.1080/10671315.1976.10615396
Shadish, W. R., Cook, T. D., & Campbell, D. T. (2002). Experimental and Quasi-experimental Designs for Generalized Causal Inference. Houghton Mifflin.
So, R. H. Y., Ho, A., & Lo, W. T. (2001). A metric to quantify virtual scene movement for the study of cybersickness: Definition, implementation, and verification. Presence: Teleoperators and Virtual Environments, 10(2), 193–215.
Stanney, K. M., Hale, K. S., Nahmens, I., & Kennedy, R. S. (2003). What to Expect from Immersive Virtual Environment Exposure: Influences of Gender, Body Mass Index, and Past Experience. Human Factors, 45(3), 504–520. https://doi.org/10.1518/hfes.45.3.504.27254
Stanney, K. M., & Hash, P. (1998). Locus of User-Initiated Control in Virtual Environments: Influences on Cybersickness. Presence: Teleoperators and Virtual Environments, 7(5), 447–459. https://doi.org/10.1162/105474698565848
Vinson, N. G., Lapointe, J.-F., Parush, A., & Roberts, S. (2012). Cybersickness induced by desktop virtual reality. In Proceedings of the 2012 Graphics Interface Conference (pp. 1–7). Retrieved from http://nparc.cisti-icist.nrc-cnrc.gc.ca/npsi/ctrl?action=rtdoc&an=20262879
Wingfield, N. (2015, March 4). To Bring Virtual Reality to Market, Furious Efforts to Solve Nausea. The New York Times. Retrieved from http://www.nytimes.com/2015/03/05/technology/solution-to-nausea-puts-virtual-reality-closer-to-market.html